Sunday, December 19, 2010
Wednesday, October 13, 2010
Thursday, September 16, 2010
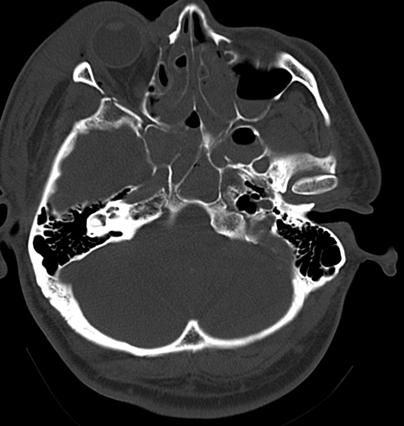
Compound Comminuted Depressed Frontoorbital Fracture
14yo Malay Boy
No known medical illness
Alleged MVA around 2am early morning
Claimed was MB vs MB (MB loss control & hit the fence, pt was not wearing helmet)
No LOC, noted bleeding from laceration wound over the scalp
No ENT bleed/ othorrhoea/ rhinorrhoea
No vomiting
No seizure
No limb weakness
No SOB/ chest pain/ abdominal pain
o/e:
Alert, conscious
GCS 15/15
Pupils 3/3 ++
Noted laceration wound (T+S done in HTAR) - about 5cm
Another laceration wound Rt temporal region (T+S done in HTAR) - 4cm
Chest/ pelvic spring done : -ve
No neck tenderness
Noted left UL- on immobilizer
BP 116/68
HR 76
Afebrile
Lungs: clear
CVS: DRNM
P/a: soft, nontender
Power Rt UL/ bilateral LL: 5/5
Sensation intact
CT brain:


CT brain:
Rt frontal depresses skull fracture -involving double table extending to superior orbital wall
No obvious ICB/ EDH/ SDH/ SAH seen
BC intact
Emergency elevation of depressed skull fracture
Frontal bone osteotomy done by neuro team with depressed fracture fragment (Lateral portion of the supraorbital rim) attached on the Rt
Depressed fragment elevated and held in place with 4 hole plate and 3 X 5mm screws
Frotal bone segment replaced and secured with horizontal long 16 hole plate across the R supraorbital rim with 5 X 5mm and 1X 4mm screws
All plates and screws from 1.5mm Walter lawrence system - straight reg.
Handed over to neuro team for closure
Post op CT scan:



No known medical illness
Alleged MVA around 2am early morning
Claimed was MB vs MB (MB loss control & hit the fence, pt was not wearing helmet)
No LOC, noted bleeding from laceration wound over the scalp
No ENT bleed/ othorrhoea/ rhinorrhoea
No vomiting
No seizure
No limb weakness
No SOB/ chest pain/ abdominal pain
o/e:
Alert, conscious
GCS 15/15
Pupils 3/3 ++
Noted laceration wound (T+S done in HTAR) - about 5cm
Another laceration wound Rt temporal region (T+S done in HTAR) - 4cm
Chest/ pelvic spring done : -ve
No neck tenderness
Noted left UL- on immobilizer
BP 116/68
HR 76
Afebrile
Lungs: clear
CVS: DRNM
P/a: soft, nontender
Power Rt UL/ bilateral LL: 5/5
Sensation intact
CT brain:


CT brain:
Rt frontal depresses skull fracture -involving double table extending to superior orbital wall
No obvious ICB/ EDH/ SDH/ SAH seen
BC intact
Emergency elevation of depressed skull fracture
Frontal bone osteotomy done by neuro team with depressed fracture fragment (Lateral portion of the supraorbital rim) attached on the Rt
Depressed fragment elevated and held in place with 4 hole plate and 3 X 5mm screws
Frotal bone segment replaced and secured with horizontal long 16 hole plate across the R supraorbital rim with 5 X 5mm and 1X 4mm screws
All plates and screws from 1.5mm Walter lawrence system - straight reg.
Handed over to neuro team for closure
Post op CT scan:



Friday, August 13, 2010
Traumatic Intracerebral Hemorrhage
44 years old Malay gentle man
Alleged MVA today at Rawang
he was riding a MB before he hit a nearby old tyre by the roadside and skidded
he's wearing a fastened helmet
found unconscious and was brought alone by ambulance
Upon arrival to ED GCS was 5/15 ( E1V1M3)
pupil- rt 6mm lt 2mm fixed
patient was intubated-->noted loss of blood in the oral cavity
ryles tube inserted-->no blood/fluids come out
Pt is intubated and sedated
vital sign
BP 163/57 not on inotrops
pr 55
RR 15 on ventilator
swollen right supra-orbital with hematoma
pupil Rt cannot be asscess, Lt 2mm, non reactive
No oozing of blood from ear and nose
Noted dry blood over the nose and left ear
 Emergency CT scan brain:
Emergency CT scan brain:
ICB at Left frontal 5x4 cm over 4 cut with midline shift 0.6cm
no hydrochepalus, brain appears tight
Urgent craniectomy and evacuation of blood clot was performed.
 Subsequently percutaneous tracheostomy was performed and weaned off ventilator
Subsequently percutaneous tracheostomy was performed and weaned off ventilator
Currently CGS E4VTM5
Alleged MVA today at Rawang
he was riding a MB before he hit a nearby old tyre by the roadside and skidded
he's wearing a fastened helmet
found unconscious and was brought alone by ambulance
Upon arrival to ED GCS was 5/15 ( E1V1M3)
pupil- rt 6mm lt 2mm fixed
patient was intubated-->noted loss of blood in the oral cavity
ryles tube inserted-->no blood/fluids come out
Pt is intubated and sedated
vital sign
BP 163/57 not on inotrops
pr 55
RR 15 on ventilator
swollen right supra-orbital with hematoma
pupil Rt cannot be asscess, Lt 2mm, non reactive
No oozing of blood from ear and nose
Noted dry blood over the nose and left ear

 Emergency CT scan brain:
Emergency CT scan brain:ICB at Left frontal 5x4 cm over 4 cut with midline shift 0.6cm
no hydrochepalus, brain appears tight
Urgent craniectomy and evacuation of blood clot was performed.
 Subsequently percutaneous tracheostomy was performed and weaned off ventilator
Subsequently percutaneous tracheostomy was performed and weaned off ventilatorCurrently CGS E4VTM5
Wednesday, July 14, 2010
Traumatic C2 dens fracture (Type II)
16 years old Chinese gentlemen, with no known medical illness
He was alleged MVA on 24/4/10 at 11 am in Klang.
He was a back seat passenger of a car with another 3 friends, while on the way to work.
The car was collided with a lorry.
LOC with unknown exact duration.
He was brought to HTAR with an ambulance. All other three victims died at the scene.
Upon arrival at HTAR, GCS was 7/15 then improved to 12/15 on the same day
Able to move all limbs and had 2 episodes of vomiting upon arrival
On arrival at Neurosurgical Centre;
He was on cervical collar
conscious, alert
GCS: E3V4M6
pupils:3/3 reactive ( left periorbiotal hematoma, cornea looks clear but conjunctiva hemorrhage seen)
L/W over the left frontal region --> T&S done in HTAR
multiple abrasion wound over the face
BP: 120/87
HR: 94
temp:37
SPO2: 100% on air
CT scan brain : Bifrontal contusion with comminuted frontal bone fracture with the involvement of frontal air sinuses (anterior and posterior wall) and thin left frontal EDH


 Cervical X-ray shows C2 odontoid fracture
Cervical X-ray shows C2 odontoid fracture



 MRI cervical shows anterior displacement of dens with normal cervical cord
MRI cervical shows anterior displacement of dens with normal cervical cord


CT cervical shows type II odontoid fracture.




 He was subjected to odontoid screw placement. Intra-operatively, reduction of displacement was done guided by the image intensifier. Post-operatively, he was extubated with no neurological deficit.
He was subjected to odontoid screw placement. Intra-operatively, reduction of displacement was done guided by the image intensifier. Post-operatively, he was extubated with no neurological deficit.
Post-op Cervical X-rays show the position of the screw.


He was alleged MVA on 24/4/10 at 11 am in Klang.
He was a back seat passenger of a car with another 3 friends, while on the way to work.
The car was collided with a lorry.
LOC with unknown exact duration.
He was brought to HTAR with an ambulance. All other three victims died at the scene.
Upon arrival at HTAR, GCS was 7/15 then improved to 12/15 on the same day
Able to move all limbs and had 2 episodes of vomiting upon arrival
On arrival at Neurosurgical Centre;
He was on cervical collar
conscious, alert
GCS: E3V4M6
pupils:3/3 reactive ( left periorbiotal hematoma, cornea looks clear but conjunctiva hemorrhage seen)
L/W over the left frontal region --> T&S done in HTAR
multiple abrasion wound over the face
BP: 120/87
HR: 94
temp:37
SPO2: 100% on air
CT scan brain : Bifrontal contusion with comminuted frontal bone fracture with the involvement of frontal air sinuses (anterior and posterior wall) and thin left frontal EDH


 Cervical X-ray shows C2 odontoid fracture
Cervical X-ray shows C2 odontoid fracture


 MRI cervical shows anterior displacement of dens with normal cervical cord
MRI cervical shows anterior displacement of dens with normal cervical cord

CT cervical shows type II odontoid fracture.




 He was subjected to odontoid screw placement. Intra-operatively, reduction of displacement was done guided by the image intensifier. Post-operatively, he was extubated with no neurological deficit.
He was subjected to odontoid screw placement. Intra-operatively, reduction of displacement was done guided by the image intensifier. Post-operatively, he was extubated with no neurological deficit.Post-op Cervical X-rays show the position of the screw.


Saturday, July 3, 2010
Tuesday, March 30, 2010
Friday, February 26, 2010
Metastatic Squamous Cell Carcinoma
•53 Years old Gentleman
Chronic smoker with underlying COAD
Developed progressive left sided limbs weakness for 2 months, associated with headache.
No other symptoms on systemic review
GCS full, PEARL
Higher mental function intact
No cranial nerves deficit noted
Left hemiparesis 4/5 with no sensory impairment
No cerebellar sign
Other examinations - Normal
MRI showed homogenous enhancing lesion at right motor cortex, left insular and left cerebellum
Chronic smoker with underlying COAD
Developed progressive left sided limbs weakness for 2 months, associated with headache.
No other symptoms on systemic review
GCS full, PEARL
Higher mental function intact
No cranial nerves deficit noted
Left hemiparesis 4/5 with no sensory impairment
No cerebellar sign
Other examinations - Normal
MRI showed homogenous enhancing lesion at right motor cortex, left insular and left cerebellum




Tumour markers done – within normal value
CXR - NAD
CT thorax and abdomen - NAD
• Right parietal craniotomy and excision of tumour done under IGS transsulcus approach
Right parietal craniotomy and excision of tumour done under IGS transsulcus approach

 Right parietal craniotomy and excision of tumour done under IGS transsulcus approach
Right parietal craniotomy and excision of tumour done under IGS transsulcus approach
Post-operatively, his weakness remain same.
On follow-up 2 weeks after surgery his weakness improved
HPE = Metastatic squamous cell carcinoma



Subscribe to:
Comments (Atom)